While wet AMD has more direct medical treatments, understanding both forms of macular degeneration is the key to actively preserving your vision and turning fear into empowerment.
- Dry AMD involves cellular waste buildup (drusen) and is primarily managed with proactive lifestyle choices and specific nutritional supplements like AREDS2.
- Wet AMD involves abnormal blood vessel growth, causes faster vision changes, and is treated with timely eye injections to stabilize and preserve sight.
Recommendation: Use this knowledge not to worry, but to build a strong partnership with your eye specialist and create a proactive vision roadmap.
Hearing the words “macular degeneration” can feel like a closing door. It’s a moment that can feel isolating, filled with uncertainty and a deep-seated fear of losing not just your sight, but your independence. You might be wondering what this means for reading your favorite books, recognizing the faces of your grandchildren, or simply navigating your own home. The medical terms—dry, wet, drusen, anti-VEGF—can sound like a foreign language, adding to the anxiety. Many articles simply list symptoms or offer generic advice, but they miss the most important point: the person behind the diagnosis.
This is where we shift the conversation. This diagnosis is not a final verdict. Think of it instead as the beginning of a new map—a vision roadmap. The key to navigating this journey successfully isn’t just about knowing what treatments exist; it’s about understanding the “why” behind your specific condition. By learning how dry and wet AMD work at a cellular level, you transform from a passive patient into an empowered, active partner in your own care. This article is designed to give you that power. We will demystify the science, clarify the treatments, and provide you with concrete, proactive steps you can take starting today to protect and preserve the vision you have.
For those who prefer a visual summary, the following video offers a compassionate look into living with macular degeneration, sharing stories of hope and adaptation that complement the practical guidance in this article.
To help you navigate this comprehensive guide, we have structured the information into clear, focused sections. The summary below provides a direct path to each topic, allowing you to explore the aspects of AMD that matter most to you right now.
Summary: Your Guide to Navigating an AMD Diagnosis
- Why Cellular Waste Buildup Destroys Central Vision Over Time?
- How to Use High-Contrast Labeling in the Kitchen for AMD Safety?
- AREDS 1 or AREDS 2:Understanding 20/20 Vision: Why Perfect Acuity Doesn’t Guarantee Eye Health
- The Cumulative UV Effect: Why Sunglasses at 20 Protect Your Macula at 70
- When to Treat: Recognizing the Shift From Dry to Wet AMD Instantly
- Why Quitting Smoking Reduces Your Risk of Cataracts by 40%?
- Injections or Surgery: Which Is Best for a Macular Hole?
- How to Use an Amsler Grid on Your Fridge to Check for Distortion?
Why Cellular Waste Buildup Destroys Central Vision Over Time?
To truly understand dry AMD, it helps to think of your retina—the light-sensitive tissue at the back of your eye—as an incredibly busy city. The photoreceptor cells that allow you to see are working nonstop, generating energy and, consequently, waste products. A healthy eye has an efficient sanitation system, a process called autophagy, that cleans up this cellular debris. This is a form of cellular housekeeping that keeps the retina pristine. However, with age, this cleanup process can become less effective.
When this waste isn’t removed properly, it builds up into small, yellow deposits called drusen. According to research published in 2024 demonstrates that these drusen are composed of damaged proteins and lipids. At first, small drusen may not affect your vision at all. But as they grow in size or number, they begin to damage the vital retinal pigment epithelium (RPE) cells responsible for nourishing your photoreceptors. This damage is what leads to the gradual blurring or distortion of your central vision, the hallmark of dry AMD.
The “Garbage Disposal” Analogy for Retinal Health
Research from the National Institutes of Health (NIH) provides a powerful analogy. As one scientist noted, the lysosomes within RPE cells are like the cell’s “garbage disposals.” A study investigating a specific protein, AKT2, found that when this protein was overactive, the lysosomes stopped working correctly. This malfunction led to the RPE cells degenerating and the development of dry AMD symptoms in mouse models. This discovery highlights how crucial the eye’s internal cleanup system is and offers a potential target for future therapies aimed at fixing this impaired proteostasis.
This process is why dry AMD is often a slow, progressive condition. The damage accumulates over years as the cellular housekeeping falls further and further behind. Understanding this mechanism is the first step in your vision roadmap, as it explains why lifestyle and nutritional interventions are so critical—they are designed to support this very cleanup system.
How to Use High-Contrast Labeling in the Kitchen for AMD Safety?
As central vision becomes less clear, everyday tasks can become frustrating and even hazardous. The kitchen, with its sharp utensils, hot surfaces, and small-print packaging, presents unique challenges. However, you can reclaim your confidence and safety in this space through a simple yet powerful strategy: enhancing contrast. Your brain relies on contrast to distinguish objects, and by making these differences more dramatic, you give your eyes the best possible chance to see clearly.
This isn’t about a complete renovation; it’s about smart, targeted modifications. Start by identifying the most crucial items and areas. Use bold, black markers on white labels for spice jars and canisters. Apply brightly colored tape—like yellow or red—to the edges of countertops and steps. For appliances, small, raised tactile dots placed on key settings (e.g., ‘350°’ on the oven, ‘High’ on the microwave) can provide both visual and touch-based cues.

As the image above illustrates, these modifications don’t have to be clinical or ugly. A well-organized, high-contrast kitchen can look modern and intentional. The goal is to create a predictable, easily navigable environment. Using different colored cutting boards—one white for onions, one dark green for bell peppers—can make food preparation safer and less strenuous on your eyes. These small acts of proactive management reduce daily strain and significantly boost your independence.
AREDS 1 or AREDS 2:Understanding 20/20 Vision: Why Perfect Acuity Doesn’t Guarantee Eye Health
One of the most confusing aspects of an early AMD diagnosis is that you might still have 20/20 vision on an eye chart. This can create a false sense of security. It’s crucial to understand that visual acuity—the ability to see letters on a chart—is only one measure of eye health. You can have a perfectly healthy macula with poor acuity, or you can have perfect 20/20 acuity with early signs of AMD, like drusen, already present. Your macula is responsible for your central, detailed vision, and it can be undergoing changes long before it affects your ability to pass a standard vision test.
This is why proactive nutritional support is a cornerstone of managing dry AMD. The Age-Related Eye Disease Studies (AREDS and AREDS2) were landmark clinical trials that identified a specific combination of vitamins and minerals that can slow the progression of intermediate-to-advanced AMD. The original AREDS formula was effective, but the updated AREDS2 formula is now the standard of care for a critical reason.
AREDS2 investigators tested the effect of eliminating beta-carotene, which in some studies increased lung cancer risk in smokers.
– National Eye Institute, AREDS/AREDS2 Clinical Trials
The AREDS2 formula replaced beta-carotene with lutein and zeaxanthin, two powerful antioxidants that are naturally found in the macula. Not only is this formula safer for current and former smokers, but a 2022 long-term study revealed that adding lutein and zeaxanthin provided an additional 10% risk reduction in progression to late AMD compared to the original formula. These supplements are not a cure, but they are a scientifically-proven tool in your vision preservation toolkit, helping to protect the macula’s delicate cells from further damage.
The Cumulative UV Effect: Why Sunglasses at 20 Protect Your Macula at 70
Just as skin needs protection from the sun, so do your eyes. The damage from ultraviolet (UV) radiation is cumulative, meaning it builds up over a lifetime. The sunlight you were exposed to in your 20s and 30s contributes to the health of your macula in your 60s, 70s, and beyond. High-energy UV and blue light can generate oxidative stress in the retina, accelerating the aging processes that contribute to AMD. Protecting your eyes from the sun is one of the most powerful and simple proactive steps you can take, regardless of your age or diagnosis.
However, not all sunglasses are created equal. The darkness of the lens has nothing to do with its level of UV protection. You need to become an informed consumer to ensure you’re getting real protection, not just shade. Think of it as investing in medical equipment for your eyes. The right pair of sunglasses is a non-negotiable part of your daily routine, just like any medication you might take. It’s an active step in your vision preservation plan.
Choosing the right lenses can feel overwhelming, but it boils down to a few key features. Use the following checklist as your guide the next time you shop for sunglasses to ensure you are giving your macula the best possible defense against harmful radiation.
Your Action Plan: Expert Lens Shopping Guide for UV Protection
- Verify Certification: Look for a label that explicitly states “UV400” or “100% UV protection.” This is the most critical feature.
- Maximize Coverage: Choose wraparound styles or large frames that fit snugly to block peripheral rays from entering around the edges.
- Enhance Contrast: Consider amber, copper, or brown tints. These colors can improve contrast, which is especially helpful for people with AMD, without sacrificing protection.
- Filter Blue Light: Ask about lenses with blue-light filtering capabilities for an added layer of protection against high-energy visible (HEV) light.
- Cut the Glare: Ensure lenses are polarized, especially if you spend time near water, snow, or driving, as they dramatically reduce reflective glare.
When to Treat: Recognizing the Shift From Dry to Wet AMD Instantly
For the approximately 10-15% of individuals with AMD, the condition can transition from the dry form to the more aggressive wet form. This is the most critical junction in your vision roadmap, where immediate action can make all the difference. While dry AMD is characterized by the slow buildup of drusen, wet AMD occurs when the body tries to “fix” the damaged retina by growing new, fragile blood vessels under the macula. This process is called choroidal neovascularization (CNV).
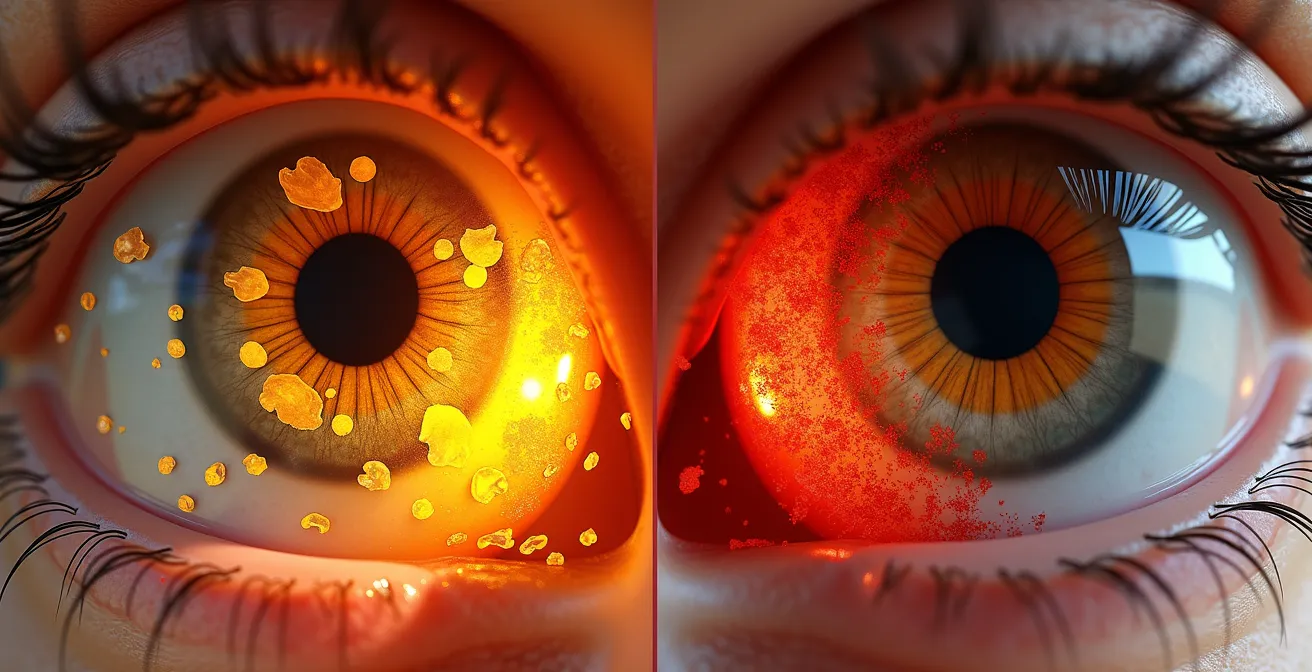
These new vessels are weak and abnormal. They leak blood and fluid into the retina, causing rapid and severe damage to the photoreceptor cells. This is why the National Eye Institute confirms that wet AMD usually leads to faster and more significant central vision loss than dry AMD. The key symptom signaling this shift is a sudden change in your vision, particularly the appearance of metamorphopsia—where straight lines appear wavy, bent, or distorted. You might also notice a new, persistent blind spot (scotoma) in your central vision.

As the image powerfully conveys, this distortion is a direct result of fluid lifting and warping the normally flat surface of the macula. Unlike dry AMD, for which treatments are primarily preventative, wet AMD has direct medical treatments. The standard of care is a series of injections of a medicine called anti-VEGF (anti-vascular endothelial growth factor) directly into the eye. This sounds frightening, but the procedure is quick, and the eye is numbed completely. This medicine blocks the signal that tells the body to grow these leaky vessels, often causing them to shrink and the fluid to dry up. Timely treatment can stop further vision loss and, in some cases, even restore some lost sight.
Why Quitting Smoking Reduces Your Risk of Cataracts by 40%?
While this article focuses on AMD, it’s essential to understand that major risk factors for one eye disease often impact others. Smoking is arguably the single most significant controllable risk factor for eye health. The headline mentions cataracts, but the link between smoking and AMD is even stronger and more direct. Smokers are up to four times more likely to develop AMD than non-smokers.
The toxins in cigarette smoke enter your bloodstream and travel throughout your body, including to the delicate structures of the eye. They create massive oxidative stress, damaging cells and impairing blood flow to the retina. This directly accelerates the aging processes that lead to drusen formation and the potential shift to wet AMD. If your eye is a busy city (as in our earlier analogy), smoking is like a constant stream of pollution that chokes the sanitation systems and corrodes the infrastructure.
The most empowering message here is one of hope and control. The damage is not necessarily permanent. Making the decision to quit, even after a diagnosis, can have a profound impact on the future of your vision. It is a powerful step on your proactive vision roadmap.
Hope for Former Smokers: Risk Reduction After Quitting
It’s never too late to make a difference. Observational studies show that the risk for AMD in former smokers begins to decrease over time, eventually becoming only slightly higher than for those who have never smoked. For a person who already has AMD in one eye, quitting smoking is one of the most important actions they can take to protect the other eye. It is a tangible, powerful way to reclaim agency over your health.
Quitting is incredibly difficult, but resources are available. Speak with your primary care physician about cessation programs, nicotine replacement therapies, and support groups. Framing this decision as a direct action to save your sight can provide powerful motivation.
Injections or Surgery: Which Is Best for a Macular Hole?
As you navigate your AMD diagnosis, you will hear terms like “eye injections” and “eye surgery.” It’s easy for these to become jumbled, causing unnecessary anxiety. One common point of confusion is the difference between treatments for wet AMD and treatments for a completely different condition: a macular hole. While both affect the macula and your central vision, they are fundamentally different problems with different solutions. Empowering yourself means learning to distinguish between them.
A macular hole is a small, physical tear or break in the macula, often caused by the vitreous gel inside the eye pulling away as we age. Wet AMD, as we’ve discussed, is a disease process involving leaky blood vessels beneath the retina. The treatments are therefore completely distinct. Wet AMD is managed with ongoing anti-VEGF injections in an office setting. A macular hole is typically repaired with a one-time surgery in an operating room called a vitrectomy.
During a vitrectomy for a macular hole, the surgeon removes the vitreous gel and places a gas bubble in the eye to act as a temporary bandage, pressing the edges of the hole flat to help it heal. This often requires a period of face-down recovery. The following table, based on information from the American Academy of Ophthalmology, clarifies the key differences.
| Aspect | Macular Hole Treatment | Wet AMD Treatment |
|---|---|---|
| Primary Approach | Vitrectomy surgery (90% cases) | Anti-VEGF injections |
| Procedure Setting | Operating room | Office procedure |
| Recovery Time | 2-8 weeks with face-down positioning | 1-2 days minimal restrictions |
| Treatment Frequency | Usually one-time surgery | Monthly to quarterly injections |
| Success Rate | 90% hole closure rate | 90% stabilization/improvement |
Knowing this difference is important. If you are diagnosed with wet AMD, your treatment path will involve injections, not the kind of surgery and recovery associated with a macular hole. This clarity can significantly reduce anxiety about what to expect.
Key takeaways
- Dry AMD is a ‘housekeeping’ problem of cellular waste (drusen); Wet AMD is a ‘plumbing’ problem of leaky blood vessels.
- Proactive management for dry AMD focuses on nutrition (AREDS2), UV protection, and not smoking.
- The sudden onset of wavy lines (metamorphopsia) is a medical emergency signaling a potential shift to wet AMD, which requires immediate treatment with injections.
How to Use an Amsler Grid on Your Fridge to Check for Distortion?
The single most powerful tool you have for proactive monitoring is a simple black-and-white pattern of lines: the Amsler grid. This grid is your personal, daily early-warning system for detecting the shift from dry to wet AMD. Using it correctly and consistently transforms you from a passive observer into the vigilant guardian of your own sight. Placing it somewhere you see every day, like on the refrigerator, makes it part of your routine.
The purpose of the grid is to test for metamorphopsia. When you look at the central dot, all the lines—both horizontal and vertical—should appear perfectly straight and unbroken. If they appear wavy, blurry, distorted, or if parts of the grid seem to be missing, it is a red flag that fluid may be accumulating under your macula. This requires an immediate call to your ophthalmologist.
To ensure your test is accurate, follow this medical-grade protocol every day:
- Position yourself about 12-15 inches away from the grid.
- If you use reading glasses, wear them for the test.
- Cover one eye completely with your hand. Never test both eyes at once.
- Stare directly at the center dot and keep your eye focused there.
- While looking at the dot, pay attention to the surrounding lines in your peripheral vision. Do you notice any wavy, broken, or missing lines?
- Repeat the process with your other eye.
- If you notice any new change, no matter how small, contact your eye doctor’s office immediately.
Bringing the Amsler Grid into the 21st Century
While a paper grid on the fridge is effective, modern technology offers enhanced tools. Smartphone applications like ‘Amsler Grid Eye Test’ provide helpful features such as automatic daily reminders, digital records of your test results with timestamps, and the ability to overlay previous tests to track changes more easily. Some even allow you to share your results directly with your doctor, facilitating remote monitoring and a stronger partnership in your care.
This simple, one-minute daily test is the cornerstone of your empowered patient journey. It puts the power of detection directly into your hands.
Your journey with AMD is not one you walk alone. This simple grid, this knowledge, and these proactive steps are your tools. The next, most important step is to take this information to your retinal specialist. Book your next appointment not with fear, but with a clear agenda to co-create your personal vision roadmap.
Frequently Asked Questions About UV Protection and Eye Health
Do darker lenses provide better UV protection?
False. Tint darkness has no correlation with UV protection. Clear lenses with a UV400 coating can provide 100% protection, while dark lenses without a proper coating may offer none at all. The protective quality is in the invisible coating, not the color.
Is UV protection unnecessary on cloudy days?
False. Up to 80% of the sun’s harmful UV rays can penetrate clouds, haze, and fog. This means eye protection is essential even on overcast days, as the cumulative damage still occurs.
Are people with dark eyes naturally protected from UV damage?
False. While a darker iris (the colored part of the eye) may offer slightly more comfort in bright light by blocking some visible light, it provides no significant protection to the macula at the back of the eye from invisible UV radiation. The risk of UV-related macular damage is independent of eye color.